Literature Review
Introduction
Dysphagia is the medical term for swallowing difficulties (Langdon and Blacker, 2010). Stroke is a condition where the blood supply to a part of the brain is disrupted (Moloney and Walshe, 2017). Approximately 50% of stroke survivors have experienced dysphagia, compared to those with Parkinson’s and multiple sclerosis. As a result of the high prevalence of stroke-related dysphagia, this literature review will be focusing on this client group (Stroke Association, 2021).
This review will be examining the impact of dysphagia on the Quality of Life (QoL) of stroke patients by reviewing eight research papers. The World Health Organisation (2022a) defines QoL in relation to an individual’s perception of their living conditions with regards to their expectations, concerns, goals, and standards. The significance of this question has been highlighted in previous studies (Carlsson et al., 2004; Jacobsson et al., 2000; Medin et al., 2010; Perry and McLaren, 2003), which primarily focused more on dysphagia symptoms and impairment and less on QoL, suggesting a possible research gap (Hellden et al., 2018).
Addressing this gap is essential because dysphagia can negatively impact QoL. For example, Drozdz et al. (2014) discovered dysphagia resulted in feelings of anxiety. Moreover, Smith et al. (2023) directly discovered from the views of adults with swallowing difficulties that dysphagia had reduced their physical safety when eating and drinking, which inevitably limited their choices and control overeating, resulting in poor mealtime experiences and social engagement. Clinicians can use this information to understand patient experiences and improve patient care and services, thus promoting multi-disciplinary work (Fernandez et al., 2013). This takes a person-centred and holistic approach because it encourages understanding clients beyond their impairment (World Health Organisation, 2022b).
This review proposes importance within the field of Speech and Language Therapy (SLT) because professionals are favoured for providing dysphagia services, with support from an inter-professional team. Therefore, this review aims to inform clinicians about how to improve difficulties related to dysphagia, whether physical or psychosocial (Royal College of Speech and Language Therapy, 2021).
A recent qualitative meta-analysis by Li et al. (2021) aimed to uncover the experiences of stroke patients with dysphagia. Although this may seem similar to this literature review, it differed in many ways. The studies included in this review provide a more up-to-date view of the experiences of patients with stroke-related dysphagia. For example, papers within the last 10 years, up to January 2022, are included, whereas Li et al. (2021) included older papers. This is important because dysphagia research is continuously evolving due to advances in technology, impacting how individuals experience dysphagia, which suggests that the findings published by Li et al. (2021) may be different to those in this review (Triggs and Pandolfino, 2019). This review also includes quantitative papers and not solely qualitative studies, unlike that of Li et al. (2021), thereby enabling broader and more thorough insights into QoL.
Al Rjoob et al. (2022) also conducted a recent review on the current literature regarding the QoL in stroke patients with dysphagia. Despite the fact that this may also seem very similar to this literature review, it was slightly different. This is because Al Rjoob et al. (2022) specifically selected papers focused on how the QoL of individuals with stroke-related dysphagia may be impacted by receiving dysphagia therapy. This literature review focuses more on the general experiences of those with stroke-related dysphagia and its impact on four aspects of QoL, including mental well-being, the environment, physical health, and personal factors, rather than intervention effectiveness. Furthermore, Al Rjoob et al. (2022), similar to Li et al. (2021), only included quantitative papers, which could limit the possibility of there being a more detailed understanding of how stroke-related dysphagia can impact QoL.
Search Strategy
This section will focus on the retrieval of papers for this review.
The PEO framework was chosen to frame the research question and search strategy because it has been commonly used for qualitative research focused on subjective experiences (Aveyard, 2019), which allow to better select studies:
P (population): Stroke patients.
E (exposure): Dysphagia post-stroke.
O (outcome): Quality of Life / patient experiences.
The creation of a research question was the initial step in conducting this literature review. The identification of key terms and synonyms was a crucial step in choosing the most appropriate terms for the research question, which helped define the terms for the search strategy. To select these, various strategies were used, such as the Medical Subject Headings (MeSH) thesaurus, an Oxford thesaurus, and broad reading to identify alternative terms (Waite, 2009). This reduced bias because thesauruses provide a variety of synonyms for a term, increasing the likelihood of finding appropriate research papers, rather than selecting terms subjectively. Moreover, MeSH provides a standardised list of subject headings, thereby increasing the number of articles discovered. Controlled key terms were also used, which involved using the databases’ own search terms to increase the number of synonyms found (Aveyard, 2019).
Combining key terms involved using the Boolean operators ‘AND’, ‘NOT’, and ‘OR’. The Boolean operator ‘AND’ helped limit the search to focus on the interconnection between dysphagia, stroke, and QoL. Similarly, ‘NOT’ limited the search number by excluding intervention-focused papers. However, ‘OR’ widened the search to include a variety of synonyms for a word. Double quotation marks were used for the term ‘’QoL’’ to instruct the database to search for the words together (Aveyard, 2019). In the databases Medline Full Text and PubMed, the following combinations of key terms were used: ‘’dysphagia’’ OR ‘’swallowing difficulties’’ OR ‘’swallowing disorders’’ AND ‘’Experience’’ OR ‘’Quality of Life’’ OR ‘’QoL’’ OR ‘’Social Participation’’ OR ‘’Pleasure’’ AND ‘’Stroke’’ OR ‘’CVA’’ OR ‘’Cerebrovascular accident’’ OR ‘’Cerebrovascular event’’ NOT ‘’Intervention’’ OR ‘’Therapy’’. The other databases were more limited and restricted; therefore, a string search using ‘’quality of life’’ AND ‘’dysphagia’’ AND ‘’stroke’’ NOT ‘’intervention’’ was applied to filter out relevant articles.
Eligibility Criteria
The inclusion criteria included English language papers, journal articles, papers published within the last 5–10 years, papers focused on stroke being the main cause of dysphagia, patient experiences, qualitative studies, quantitative studies, and peer-reviewed articles. Exclusion criteria included non-stroke dysphagia, experiences from non-dysphagia patients, intervention-related studies, and grey literature.
Study Selection
To avoid bias associated with subjectively selecting papers, keywords were made to appear in the titles and abstracts only. This was because searching for these terms to appear in the whole article resulted in an overwhelming number of papers. However, the entire volume of relevant databases was not used, reducing the reliability of the search process. To reduce this limitation, a technique known as the “snowball method” was used. This involved identifying possible papers during the database search and scanning through the reference list to identify potential articles. During this method, there was a repetition in the same articles found during the database search, highlighting that data saturation had been achieved, making it appropriate to cease the search (Aveyard, 2019).
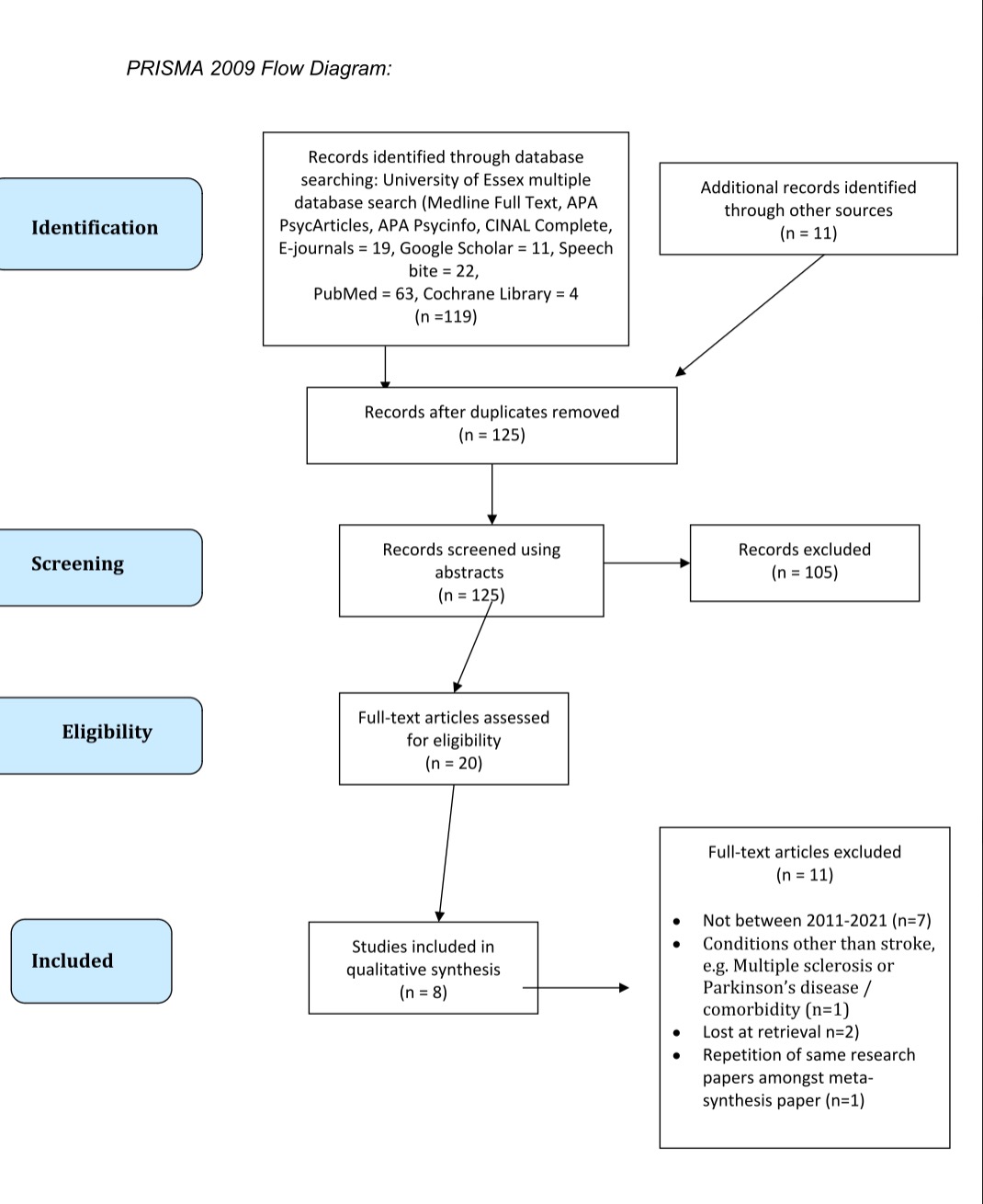
A systematic search was conducted on PubMed, Google Scholar, Medline Full Text, APA PsycArticles, APA Psycinfo, CINAL Complete, E-journals, Speech bite, PubMed, and Cochrane Library to increase the relevancy of articles (ASHA, 2022). Conducting multiple database searches evaluated the consistency of the search process. For example, there was repetition in the same articles across the different databases, suggesting high reliability in the search process. In Appendix 1, a PRISMA (2009) diagram has been provided to document the systematic overview of the steps involved during this literature search.
Summary of Results
Four qualitative and four quantitative papers were identified. The sample sizes ranged from 2 to 79 participants. The settings ranged from acute stroke units, inpatient hospitals, patients’ homes, and rehabilitation units. These studies were conducted in the United Kingdom, Denmark, Sweden, South Korea, Iran, and Brazil.
Method of Analysis
The findings of each paper were read several times to identify common themes related to the research question. Potential themes were then grouped together to analyse which papers displayed similar findings. This process is known as thematic analysis and is encouraged by Aveyard (2019) for novice researchers, compared to advanced approaches such as meta-analysis or meta-ethnography, because of the high level of expertise required. Four themes were identified: cognitive health, adaptation and coping, environmental consequences, and physiological consequences. To establish confidence that these themes were robust, each theme was checked to make sure the titles were appropriate and that the sub-themes suited the main themes, which involved manoeuvring and altering the titles until a comprehensive understanding of the findings was achieved, in a process known as comparative analysis (Braun and Clarke, 2022; Jason and Glenwick, 2016).
CASP Tools
The qualitative papers were critiqued using the qualitative Critical Appraisal Skills Programme (CASP) tool (CASP, 2021). CASP tools are well established and recommended for quality approval in health-related evidence syntheses and for novice researchers (Long et al., 2020). The quantitative papers were critiqued using the Joanna Briggs Institute (JBI) critical appraisal checklist for cross-sectional studies (Joanna Briggs Institute, 2017). The JBI tool is an established tool praised by clinicians for providing detail and a rationale for the questions asked (Aveyard, 2019; Holland and Rees, 2010).
Thematic Analysis
This section will be comparing and contrasting the findings in relation to addressing the research question.
Physiological Consequences
Stroke-related dysphagia can cause physiological consequences, such as recurrent pneumonia, throat clearing, and repetitive swallowing, which have been shown to impact the QoL of individuals (Moloney and Walshe, 2017). Moloney and Walshe (2017) conducted a qualitative study using autobiographical accounts to explore the personal experiences of 10 individuals with stroke-related dysphagia. The findings demonstrated that oral structure abnormalities decreased QoL. This can be supported by a quantitative study by Hong and Yoo (2017) that used the swallowing QoL (SWAL-QoL) to compare swallowing function and QoL in 79 stroke patients with dysphagia. However, they discovered that better anatomical oral structures improved swallowing function due to personal factors such as high motivation, which increased QoL.
To have a clearer understanding of these structural abnormalities, Kjaersgaard and Pallesen (2020) used semi-structured interviews to explore the experiences of two individuals with brain-stem stroke-related dysphagia and identified that these anatomical structure abnormalities involved constant saliva production, coughing attacks, and pneumonia, which resulted in both individuals struggling to eat and drink due to atypical changes in sensation and taste of the tongue. Similarly, in a qualitative study that conducted unstructured interviews to investigate how stroke-related dysphagia impacts daily living, Hellden et al. (2018) uncovered that dysphagia resulted in weight loss, difficulty with managing saliva, and taste changes. Although the findings are similar, both studies included small sample sizes, which may have limited the generalisability of the findings to a whole stroke population (Faber and Fonseca, 2014). Nevertheless, Hellden et al. (2018) argued the findings could be applied to other populations because symptoms in oropharyngeal dysphagia are similar in other neurological conditions. However, Aveyard (2019) would disagree and argue that classifying a qualitative study’s sample size as small is based on quantitative frameworks, because in qualitative research to achieve replicability and generalisability, data saturation would need to be achieved. Hellden et al. (2018), however, did not mention achieving data saturation. Alternatively, Kjaersgaard and Pallesen (2020) explained that data saturation was avoided because the inclusion of additional participants until saturation would have added more experiences, resulting in possible alterations of the findings and conclusions.
On the other hand, Martin-Harris and Jones (2008) would argue that it would have been more appropriate to use standardised measures to assess physiological symptoms, such as a Videofluoroscopy, the gold standard diagnostic tool for oropharyngeal dysphagia; a glossary for specialist terms can be seen in Appendix 2 (Martin-Harris and Jones, 2008). For example, Kim et al. (2020) used a standardised measure to conduct a retrospective, cross-sectional study where 75 stroke patients with dysphagia participated in the SWAL-QoL questionnaire. A correlation between the SWAL-QoL and Videofluoroscopic dysphagia score (VDS), which is used to predict the long-term prognosis of stroke-related dysphagia, was obtained. The findings from the VDS score illustrated that as pharyngeal function decreases, QoL also decreases. This suggests that the severer the physiological consequences of dysphagia, the greater impact on QoL. This deduction was supported by Bakhtiyari et al. (2020), who conducted a cross-sectional study investigating the impact of dysphagia on QoL in 60 Iranian stroke survivors using the Dysphagia Handicap Index (DHI), which determined the impact of dysphagia on QoL, and found that the severer the dysphagia, the greater impact on QoL.
Kim et al. (2020) also found in the SWAL-QoL subdomains ‘fatigue’ and ‘sleep’ that patients scored very lowly (45.27 ± 21.94) compared to those in other domains, such as social functioning, which had scores of 54.19 ± 35.32. Similarly, Pontes et al. (2017) conducted a cross-sectional study using the SWAL-QoL to examine the QoL of 35 stroke patients with dysphagia. The questionnaire illustrated that dysphagia negatively impacted sleep (43.9) and fatigue (45.7). Thus, both studies confirm the impact of physiological consequences on QoL. Both researchers can be praised for choosing the SWAL-QoL, the gold standard for determining QoL for individuals with dysphagia, with good internal consistency and reproducibility (McHorney et al., 2002). These findings may further highlight that using more standardised measures for assessing the physiological symptoms of dysphagia could increase the trustworthiness of the findings or be interpreted as confirming the findings from the earlier qualitative studies mentioned above.
Environmental Consequences
Although physiological abnormalities have been shown to impact QoL, Threats (2007) emphasised that the interconnectedness between biological and environmental factors would provide a better understanding of the impact of dysphagia on QoL. For example, Kjaersgaard and Pallesen (2020) discovered that physiological consequences, such as coughing attacks, minimised patients’ participation in social activities. Some participants would actively choose which social events to attend and avoid. However, the researchers acknowledged that sufficient data were not present to support this finding. As a result, triangulation was undertaken to increase credibility (Carter et al., 2014). Similarly, Hellden et al. (2018) found participants would avoid social situations because of the unpredictable nature of dysphagia symptoms, which resulted in difficulty maintaining intimate relations with friends and family. Eltringham et al. (2019) also discovered that one participant chose not to drink tea anymore. However, Moloney and Walshe’s (2017) findings were slightly different, explaining that others in the environment would avoid inviting participants to social occasions, rather than patients excluding themselves. Both Kjaersgaard and Pallesen (2020) and Moloney and Walshe (2017) explained this is because of the negative impact of others’ perception of dysphagia. For example, a participant explained the fear of conversing and coughing simultaneously was due to others becoming repulsed. As a result, both studies found patients would choose to eat alone and isolate themselves from society, demonstrating that an unsupportive environment could cause social isolation, thereby decreasing QoL.
It should be noted that Eltringham et al.’s (2019) study took place in the same hospital that the primary researcher worked in, leading to possible researcher bias because the author may have previously had contact with the sample population; therefore, the researcher did not recruit participants who they may have had direct clinical contact with. Despite this, credibility was still compromised due to the researcher being an SLT, which may have blurred the boundaries of being a clinician and researcher (Noble and Smith, 2015).
Despite others excluding patients from social activities, as mentioned in Moloney and Walshe’s (2017) study, some patients attempted to reintegrate back into society to reduce social isolation and better social relations, thereby increasing their QoL (Moloney and Walshe, 2017). These findings can be praised for demonstrating inter-rater reliability because two researchers examined the data, and if there were disagreements, then this was resolved through discussion, reducing researcher bias (Scheel et al., 2018). Bias was further reduced because there was no presence of a researcher when the autobiographies were written, increasing the credibility of the findings. However, a level of bias was still present as autobiographies are mostly written with an audience in mind, hindering the truth of the accounts expressed. Moreover, two authors were journalists, which could suggest a hidden motive for wanting to publish and write autobiographical texts (Krans et al., 2013). Hellden et al. (2018) also had more than one researcher analyse the findings but chose not to analyse the findings together because other interpretations could have been made, which may have limited the validity of the findings if all interpretations were not considered (Tonon, 2015).
A phenomenon known as ‘role reversal’ was also common. This was present in Moloney and Walshe’s (2017) and Eltringham et al.’s (2019) studies, explaining that participants prior to having dysphagia experienced a complete reversal in social roles by becoming dependent on others, which impacted their dignity, thereby decreasing their QoL. This impact on social functioning was also seen in Kim et al. (2020), Pontes et al. (2017), and Hong and Yoo’s (2017) studies. This suggests that stroke-related dysphagia not only affects patients but also others in the environment.
Cognitive Health
Some papers have discussed the impact of stroke-related dysphagia on patients’ cognitive health. Bakhtiyari et al. (2020) demonstrated that dysphagia negatively impacted participants’ emotional state, decreasing QoL. However, there was no control group to compare QoL between stroke patients with and without dysphagia, which would have been important to confirm the results were due to the manipulation of the independent variables and not extraneous variables (Pithon, 2013).
Pontes et al. (2017), Kim et al. (2020), and Hong and Yoo (2017) used the SWAL-QoL to quantitatively measure the impact of dysphagia on QoL. Pontes et al. (2017) demonstrated a severe impact of dysphagia on mental health, obtaining a mean score of 47.6. Hong and Yoo (2017) also demonstrated that mental health was negatively impacted by dysphagia. These researchers also sampled participants into two groups (oral-intake and non-oral-intake), where scores were obtained for both groups. The oral-intake group scored significantly higher (20.00 ± 4.30) than the non-oral-intake group (13.54 ± 6.03), suggesting mental health is better in those with less severe dysphagia, thereby bettering QoL. Similarly, Kim et al. (2020) demonstrated a higher score in the mental health domain for oral feeding (56.83 ± 31.78) than the tube-feeding group (55.15 ± 25.42). These findings indicate that although dysphagia decreased patients’ mental health overall, this was gravely impacted by the severity of an individual’s dysphagia, which could highlight the importance of prioritising certain client groups when carrying out risk assessments.
The findings from Kim et al. (2020) and Pontes et al. (2017) could be questioned because participants were enrolled based on retrospective accounts of presenting with dysphagia, rather than a standardised diagnostic test. This can be criticised because retrospective data are susceptible to recall and misclassification bias, decreasing the validity of the findings (Krans et al., 2013). On the other hand, Hong and Yoo (2017) used the swallowing function test, a diagnostic tool for classifying swallowing function levels, with high specificity and sensitivity, increasing the robustness of these findings.
Daher et al. (2017) would argue that qualitative methods are more appropriate for examining QoL because these methods provide deeper insight into individuals’ experiences and opinions. Eltringham et al. (2019) used interviews, which allowed participants to personally explain their feelings, such as fear or embarrassment, due to not being able to eat in front of others. This was also present in the studies by Moloney and Walshe (2017) and Kjaersgaard and Pallesen (2020), demonstrating that the negative psychosocial consequences of dysphagia decreased QoL. For example, Kjaersgaard and Pallesen (2020) and Moloney and Walshe (2017) highlighted that eating required a lot of concentration, causing patients mental fatigue, which caused these individuals to avoid social situations due to feeling embarrassed and annoyed. However, Hellden et al. (2018) and Moloney and Walshe (2017) also discovered some participants altered feeling these negative emotions with more optimistic thoughts, such as the possibility of improvement and recovery, thereby feeling hopeful, which improved their mental well-being and increased their QoL. Although randomised controlled trials are considered the gold standard for quality of evidence, they were not appropriate for discovering personal experiences; therefore, Kjaersgaard and Pallesen (2020) can be praised for justifying the use of case studies, because this methodology is recommended for investigating contemporary phenomena within real-life contexts (Daher et al., 2017).
To discuss the trustworthiness of the above findings, Eltringham et al. (2019) included patients during the interpretation of the findings, which would have made sure that the researchers made appropriate inferences during data analysis. Hellden et al.’s (2018) methodology may have needed to be strengthened because the sample did not consist of female participants, which would have increased the validity of the findings, because women are twice as likely as men to experience poor mental health (Aneshensel et al., 2013). However, there were no females that met the inclusion criteria. Similarly, Moloney and Walshe’s (2017) study encompassed significantly more men than women, limiting the applicability of the findings (Faber and Fonseca, 2014). This could propose that Eltringham et al.’s (2019) findings are more valid and well-grounded when interpreting the impact cognitive health can have on QoL.
Adjustment & Coping
Three papers demonstrated that patients chose to adjust and adopt coping methods to deal with the impact of dysphagia on their QoL. Moloney and Walshe (2017) highlighted that patients developed self-management strategies such as visual imagery, where they would only remember previous joyful experiences of eating and drinking. This demonstrates that participants learned to live and adjust with their dysphagia to improve their QoL. Similarly, Kjaersgaard and Pallesen (2020) found patients also developed self-management strategies, such as keeping food or drink in the mouth for longer to increase taste sensation and would not talk whilst eating to prevent discomforting symptoms such as coughing attacks. Furthermore, patients explained that adapting to dysphagia was necessary to live a meaningful and valued life with friends and family, thereby taking an optimistic approach to enhance their QoL. Hellden et al. (2018) also found patients would adjust social situations by choosing a seat near a door if coughing were to occur; thus, underlining that dysphagia resulted in participants having to plan ahead to prevent undesirable situations, feelings, and symptoms, increasing their QoL.
To determine more robust findings, it was important to examine whether researchers acknowledged their own biases and rationale for decision-making. This is known as ‘researcher reflexivity’, which ensures rigour (Johnson et al., 2020). The qualitative CASP tool highlighted that Moloney and Walshe (2017) explained that bias associated with the presence or direction of a researcher during data collection was unlikely because the data consisted of autobiographies. Moreover, the researchers immersed themselves during data analysis to develop a thorough understanding; however, subjectivity bias during this process was not considered. Therefore, ensuring researcher reflexivity would have increased the trustworthiness of the findings (Johnson et al., 2020). On the other hand, Hellden et al. (2018) was aware of potential biases and strived to consider the perspectives of the participants when searching for meaning during data analysis by analysing data at manifest (visible) and latent (underlying) levels, which increased the richness of the findings. Kjaersgaard and Pallesen (2020) also reduced researcher bias by obtaining an individual not involved in the study to fully transcribe patients’ words verbatim; however, the authors themselves recognised the lack of data to support these findings because data saturation was not obtained.
Discussion
Research Gap
The most significant research gap concerned the long-term impact of dysphagia on QoL. This is because patients primarily in hospitals or rehabilitation settings were targeted in the studies, with a lack of focus on those who have lived with dysphagia for a long period of time. Although Kjaersgaard and Pallesen (2020) did interview patients once in their homes, one month following injury, the authors recognised that further research would be needed to explore these experiences several years following dysphagia. Moloney and Walshe (2017) also highlighted this need. Three papers discussed the importance of examining the long-term impact of stroke-related dysphagia beyond a hospital environment (Eltringham et al., 2019; Hellden et al., 2018; Kim et al., 2020). This gap is valuable because investigating long-term consequences allows clinicians to provide long-term care services to improve QoL (Forder et al., 2017).
Implications
These findings contribute to existing knowledge regarding the current understanding of the experiences of individuals with stroke-related dysphagia. Hellden et al. (2018) underlined the need for improvements in healthcare support following discharge from a hospital setting to improve health outcomes and patients’ QoL. Pontes et al. (2017) also explained examining the impact of stroke-related dysphagia on QoL allowed clinicians to practice and acquire skills to improve the rehabilitation experiences of patients.
Kjaersgaard and Pallesen (2020) further discovered a lack of dysphagia-related knowledge amongst healthcare professionals, which is necessary for understanding the impact of dysphagia on patients’ QoL. To increase this understanding, it is suggested that SLTs educate and inform members of the multidisciplinary team regarding dysphagia symptoms, care, and management to improve interprofessional practice (Royal College of Speech and Language Therapy, 2021). Increasing healthcare professionals’ awareness of these experiences could allow clinicians to provide higher-quality and evidence-based care, ensuring holistic and patient-centred service delivery (Moloney and Walshe, 2017).
Conclusion
This literature review highlights the interconnectedness between the biological, environmental, personal, and emotional factors that greatly impact the QoL of individuals with stroke-related dysphagia. However, future research should examine the long-term impact of stroke-related dysphagia on QoL to improve long-term care services for patients, especially within community settings. This is because the above findings may only be generalisable to individuals living with post-stroke dysphagia in hospital and rehabilitation settings, as most studies have only examined patients in this environment. Therefore, it is likely that the physiological consequences of dysphagia from stroke may be different in individuals in community settings who have lived with this condition for a longer time. Thus, QoL is likely to be impacted by the length of time an individual has lived with the condition, as recovery and factors such as coping would also impact QoL (Forder et al., 2017).
Methodology
This study would take an interpretivist approach because the purpose is to gain an in-depth insight into the lived experiences of individuals with stroke-related dysphagia to develop an empathetic understanding of human action, known as ‘verstehen’. Interpretivists favour qualitative methods to allow for close interactions with respondents to grasp a detailed understanding of their experiences (Willis and Nilakanta, 2007; Engel and Schutt, 2005).
There are different forms of qualitative approaches, such as ethnography or the grounded theory approach; however, this project would take a phenomenological approach by focusing on subjective, lived experiences, as opposed to studying cultural issues (ethnography) or the development of theories (grounded theory) (Green and Thorogood, 2018).
Semi-structured interviews would be chosen because this method is favoured in qualitative research with a focus on uncovering and understanding the personal experiences of participants. Interviews would consist of a two-way dialogue between the researcher and respondent to explore participants’ feelings, thoughts, and experiences, supplemented by follow-up questions, probes, and comments to delve deeper into the topic. Semi-structured interviews would be chosen as opposed to unstructured interviews because an element of structure was still present. For example, having pre-set topic questions would allow the interviewer to remain on course and focused, minimising the amount of irrelevant information gathered. Furthermore, unlike in structured interviews, the detail and richness of data would still be obtained due to the open-ended nature, allowing participants to rephrase, clarify, and elaborate on their answers if needed (Green and Thorogood, 2018).
This study would undertake an interpretive phenomenological approach because there would be an emphasis on interpreting and understanding the long-term lived experiences of individuals with stroke-related dysphagia and not just the description of these experiences, which is the focus in descriptive phenomenological studies. Interpretive phenomenology examines the contextual features of an experience in relation to other influences, such as how well-being, employment, gender, or culture may influence the experiences of a phenomenon. Therefore, interpretative phenomenology is praised for allowing researchers to develop a deeper understanding of how participants’ context may influence the phenomenon being studied (Matua and Der-Wal, 2015).
Sample Selection
The sample target group for this study would consist of adult participants in the community living with on-going implications of stroke-related dysphagia for at least 2–5 years. Exclusion criteria would include patients with severe cognitive or communication difficulties, as this would cause difficulty with engaging and answering questions during the interview process, and patients with co-morbidities, as the focus would be solely on stroke-related dysphagia experiences. To verify information such as a stroke diagnosis, on-going implications of stroke-related dysphagia, and the presence of dysphagia, the researcher would need to access relevant medical information through participants’ general practitioners, whilst obtaining participants’ informed consent. The accuracy of medical records would be considered because Hong et al. (2015) demonstrated inaccuracies and incompleteness were commonly found in patients’ documents containing a history of their presenting illnesses. However, the authors did acknowledge the subjective nature of the term ‘completeness’ because what may be considered ‘complete’ for one doctor may be considered ‘incomplete’ for another.
Vasileiou et al. (2018) conducted a systematic analysis of qualitative health research over a 15-year period and determined the ideal sample size for interview-based studies is 12 participants. However, Dworkin (2012) suggests a range of 5–50 participants is appropriate, with no ideal number, but depends on a variety of factors such as the phenomenon being studied, saturation of data, or the sample population. Green and Thorogood (2018) stated that data saturation is the most important because it ensures the replicability of the study. The above qualitative papers in the literature review contained a sample size ranging from 2–10 participants, suggesting a feasible size, due to the cumbersome nature of transcribing and analysing interviews; however, data saturation would still need to be achieved.
Recruitment
For this study, purposeful sampling would be the most appropriate because participants would need specific characteristics for participation, such as long-term post-stroke dysphagia in the community. Methods such as random sampling would not be appropriate as it involves the random selection of individuals from different populations. Purposeful sampling is also widely used in qualitative research because it allows for the selection of information-rich cases related to the phenomenon being studied (Palinkas et al., 2015). An element of convenience sampling could also be apparent if participants were recruited based on close proximity to the researcher (Aveyard, 2019).
The above literature review highlights a research gap regarding a lack of inclusion of women’s perspectives. Therefore, it may be beneficial to also use maximum variation sampling. This would involve the researcher attempting to collect data from the widest range of perspectives to achieve a balance of genders; however, this depends on the participants identified (Green and Thorogood, 2018). For example, in Hellden et al.’s (2018) literature review, it was highlighted that obtaining women’s perspectives was not possible, as most female participants did not meet the eligibility criteria.
Recruitment would involve the researcher contacting SLT practices and organisations, such as the Stroke Association (2021) and East Suffolk and North Essex NHS Foundation Trust (ESNEFT, 2022). These services would be contacted through an email containing a letter of invitation to the study. This would allow the researcher to request the services to inform any suitable patients for the study and for the participants to contact the researcher themselves or to give consent for the researcher to contact them. Moreover, the researcher would request for the organisations to grant permission to advertise the study on their website, social media, or mailing lists to allow for volunteers to come forward. For individuals with any further questions and those seeking more detailed information, a leaflet would be provided, containing information about the aim, location, participant criteria, procedure, and potential benefits of the study. Informed consent would need to be gained to access potential participants’ medical records to verify suitability for the study.
Procedure
The interviews would be held in either a private hired community room or participants’ homes due to the sensitive nature of the topic, which may cause participants to feel vulnerable. Therefore, offering this choice would allow participants to feel more at ease. Participants would only have to participate in one 1-hour long interview; however, this could last slightly longer or shorter depending on the participants’ preference to stop or talk for longer. The researcher would need to create an interview topic guide containing a list of topics to be discussed and a few preset open questions for each topic. The researcher would then improvise follow-up questions, as semi-structured interviews are a combination of structured and unstructured interviews (Aveyard, 2019). A sample of an interview topic guide can be seen in Appendix 3, which contains a list of topics that could be discussed, such as the environment, mental well-being, and physiology, and a few preset open questions for each topic.
Ethics
This study would require ethical approval from the National Healthcare Service (NHS) if participants were recruited from ESNEFT, an NHS foundation trust. This process would involve seeking approval from the Health Research Authority (HRA), which would comprise a review by an NHS Research Ethics Committee, study-wide research governance checks by HRA staff, and an assessment of regulatory compliance (NHS Health Research Authority, 2021). This study would also need ethical approval from the University of Essex because of the involvement of human participants conducted by the University’s taught student (University of Essex, 2022a). The Stroke Association would also require the study to meet certain criteria to consider the recruitment of their members (Stroke Association, 2022a).
Psychological Harm
Possible risks of discomfort and psychological harm may be present, impacting participants’ well-being. For example, reflecting on current and past experiences of living with dysphagia may result in psychological harm (Jungmann and Witthoft, 2020). To manage the safety and well-being of participants, optional counselling by a qualified psychologist to discuss any worries would need to be offered at the end of the study. A counselling session costs up to £70 per hour (NHS, 2022). If participants would like to seek further help, direction to their general practitioner for NHS mental health services would also be provided.
Confidentiality
Participants’ demographic and medical information would need to be kept anonymous, such as by using an electronic safe secured by password protection and data encryption, and this would possibly be kept for a period of at least 5 years, as required by the University. Once anonymised, this data would likely be made available to other researchers via accessible data and public repositories and possibly used for novel purposes. However, this information would be kept fully anonymous and would not be identifiable by anyone. The intention of sharing this information publicly would be to spread awareness of these experiences to improve the quality of care received by patients with long-term post-stroke dysphagia whilst providing a means to empower participants to feel heard, valued, and respected. Audio recordings and transcripts would need to be anonymous with no personal data linked to the recordings or transcripts, which would need to immediately be destroyed and discarded after the analysis process.
Informed Consent
An information sheet would need to be constructed containing all the necessary information participants would need to make an informed decision to decide on participation in the study, such as the purpose of the study, the procedure, sample questions, and more.
Right to Withdraw
This study would be completely voluntary; therefore, participants who would suddenly decide to stop participating as part of the study, at any time without explanation or due to personal circumstances, would be respected. Participants would have the right to ask for their personal data to be withdrawn or destroyed. Moreover, participants would have the right to omit or refuse to answer any question, without experiencing any discriminatory treatment by the researcher. It is also important for the researcher to build a rapport with participants before the study because this could facilitate more open and honest answers during the interviews, which could also allow participants to feel more confident with withdrawing or refusing to answer a question (Bell et al., 2016).
Data Collection
To gather information, semi-structured interviews would be employed. This would be the most appropriate form of data collection for this study because interviews allow the researcher to ask participants questions, with opportunity to ask follow-up questions to clarify themselves or provide further detail on post-stroke dysphagia to increase the understanding of these experiences. This is in contrast to quantitative methods such as closed questionnaires and experiments, which would not be chosen because a quantitative approach would not allow the asking of open questions to allow the researcher to explore and provide a deeper insight into these experiences (Green and Thorogood, 2018).
The credibility of solely collecting information using interviews is questionable, however. This is because forgetting small details is likely, and writing notes whilst trying to remember exactly what participants have verbalised can be difficult, impacting the reliability of the information gathered. Therefore, to increase the credibility of findings, triangulation would be recommended. This would involve using multiple methods to collect data, such as an audio recorder and a transcriber (Aveyard, 2019). Audio recorders are commonly used for interviews to improve factual precision and for the researcher to focus more on listening, probing, asking follow-up questions, and maintaining eye contact to allow participants to feel listened to and respected. However, malfunction with the devices is possible, external background noise may block pieces of information, and participants’ awareness of the recordings may result in nervousness, causing them to be cautious about what they say (Rutakuma et al., 2020). Furthermore, transcribing the information would allow the researchers to easily analyse and become more immersed in the data to have a deeper understanding of participants’ experiences (McMullin, 2021). However, the transcription of interviews is highly time consuming; therefore, the researcher would benefit from employing a transcriber, which costs approximately £10 per hour (PayScale, 2022).
Data Analysis
Interpretive phenomenological analysis (IPA) would be used to analyse the data gained from the interviews. This is because IPA is recommended for studies that focus on uncovering the meaning of lived experiences through in-depth reflective inquiry. This would involve rich engagement and an interpretation of the findings and researcher by the researcher trying to understand the participants’ world and views. This type of analysis would also involve the researcher looking at participants in a non-judgemental way by setting aside their pre-understanding of the experiences of stroke-related dysphagia and opinions, a concept known as ‘bracketing’. This would allow the researcher to construct insightful interpretive accounts and a new understanding of this topic to increase awareness of the impact of long-term post-stroke dysphagia in the community within healthcare (Smith and Osborn, 2015).
Aveyard (2019) would argue that qualitative methodologies are susceptible to researcher bias due to the involvement of the researcher during the research process. This is because the contamination of the researchers’ own beliefs, experiences, and perceptions is possible and creates a barrier to understanding participants’ experiences. However, IPA acknowledges this and therefore encourages reflexivity, a process whereby the researcher acknowledges how they may potentially influence the research process. IPA specifically focuses on inter-subjective reflexivity, which focuses on discovering the relationship between the participant and researcher. Therefore, the main researcher would need to keep a reflexive journal of personal biases and assumptions to reduce researcher bias and improve the trustworthiness of the findings (Smith and Osborn, 2015).
Two research assistants would need be hired to further analyse the findings with the main researcher, which would enable discussions to ensure the analysis of the findings are interpreted and challenged. The final decision, however, would be from the main researcher. This would increase the credibility of the findings because interpretation would not be based on one human (Bryman, 2008).
Funding
Funding opportunities would need to be sought with the support of the Essex University Research and Enterprise Office team (University of Essex, 2022b). Funding would also be sought from the Stroke Association (2022b). Investigations of funding opportunities would be sought from the Royal College of Speech and Language Therapy (RCSLT) (2022a). The researcher would also need to explore what the United Kingdom Research and Innovation (2022) and National Institute for Health and Care Research (2022) have to offer.
Trustworthiness
Interviews are susceptible to social desirability bias, which refers to participants giving socially acceptable answers to please the researcher, impacting the credibility of the findings. Therefore, the interview questions would need to be asked in a neutral and open form, avoiding leading questions, whilst also reminding participants that answers would remain anonymous (Aveyard, 2019).
The researchers would need to build rapports with participants before the study to increase the likelihood of honest responses and to reduce response bias. However, the researchers’ pre-conceived views may impact the type of spontaneous questions asked; therefore, the researcher keeping a reflective diary could highlight any feelings, thoughts, and opinions to reflect on to increase the credibility of the findings (Bryman, 2008).
Participants having access to the topic guide and pre-set questions may increase the likelihood of rehearsed answers, decreasing the authenticity of the findings. However, this is essential to obtain informed consent due to the sensitive nature of the study. Moreover, Aveyard (2019) would argue that questions in advance could help participants express their answers more effectively, allowing them to feel better prepared.
Self-reported data has been criticised because such accounts may not be accurate and cannot be verified. However, the essence of an interview is to collect self-reported data; therefore, this cannot be avoided. To increase the trustworthiness of the accounts, the researcher would have accessed participants’ medical records to confirm the diagnosis of a stroke and dysphagia, increasing the credibility of the experiences. Despite this, self-reported data are susceptible to missing certain experiences (selective memory), exaggerating events, and recall bias, impacting the validity of findings (Bryman, 2008).
Dissemination
The proposed methods of dissemination would include submitting the research to be published in journals such as the International Journal of Language and Communication Disorders, a major journal that publishes SLT-related articles (Wiley Online Library, 2022). Submission could also be made to the International Journal of Stroke, which has contributed to the international stroke research community (Journal of Stroke, 2022). The research would also be submitted for possible display on the RCSLT’s professional Twitter account, RCSLT hubs, Clinical Excellence Network via email, and inclusion in the RCSLT research newsletter (Royal College of Speech and Language Therapy, 2022b).
A copy of the published research would be sent to the SLTs and organisations that referred participants to the study. Dissemination through the above methods would help maximise the uptake of the research by researchers, stakeholders, commissioners, clinicians, charities, and patients with a possible interest in the research study to increase the awareness and understanding of patients’ experiences with long-term post-stroke dysphagia in the community (Wilson et al., 2010).
Clinical Application
Despite the limitations, the National Institute of Health emphasises the importance of clinical research in enhancing patient health, extending life, and reducing health conditions and hospital admissions. Therefore, the findings from this research project would help raise awareness and provide a deeper insight into the long-term lived experiences of individuals with post-stroke dysphagia in the community (Alvins and Goldberg, 2007). Seymour (2017) highlighted that raising awareness can inform and educate individuals, influencing their beliefs, attitudes, and behaviour. For example, the findings from this study could influence how SLTs and members of the multidisciplinary team work with individuals with long-term post-stroke dysphagia and how these professionals could meet patients’ needs, which would only be possible through patient accounts, increasing their awareness and understanding, which would lead to improvements in health outcomes and patients’ QoL. This is emphasised by the Health and Care Professions Council (HCPC) (2022), which encourages clinicians to take into account service users, needs, and wishes by adopting evidence-based practice and person-centred care and consequently allowing patients to feel valued, respected, and appreciated. Moreover, as previously highlighted in the literature review, a research gap exists regarding the lack of community post-stroke experiences; therefore, the findings from this study would provide knowledge and educate others on these experiences (Eltringham et al., 2019; Hellden et al., 2018; Kim et al., 2020).
References
Al Rjoob, M., Hassan, N. F. H. N., Aziz, M. A. A., Zakaria, M. N. & Mustafar, M. F. B. M. (2022) ‘Quality of life in stroke patients with dysphagia: a systematic review’, La Tunisie medicale, 100(10), pp. 664.
Alvins, A. & Goldberg, H. (2007) ‘Creating a culture of research’, Contemporary Clinical Trials, 28(4), pp. 557–562. doi: 10.1016/j.cct.2007.02.004
Aneshensel, C. S., Phelan, J. C. & Bierman, A. (2013) Handbook of the Sociology of Mental Health. (2nd Eds) Dordrecht: Springer.
Aveyard, H. (2019) Doing a literature review in health and social care: a practical guide. (4th Eds) London: Open University Press.
Bakhtiyari, J., Dadgar, H., Maddah, M., Ghorbani, R., Charkhi, F. & Rezaee, Z. (2020) ‘The effects of dysphagia on quality of life in stroke survivors’, Middle East Journal of Rehabilitation and Health Studies, 7(4). doi: 10.5812/mejrh.105722
Bell, K., Fahmy, E. & Gordan, D. (2016) ‘Quantitative conversations: the importance of developing rapport in standardised interviewing’, Quality and Quantity, 50(1), pp. 193–212. doi: 10.1007/s11135-014-0144-2
Braun, V. & Clarke, V. (2022) Thematic analysis: a practical guide. London: SAGE Publications
Bryman, A. (2008) Social Research Methods (3rd Eds) Oxford: Oxford University Press.
Carlsson, E., Ehrenberg, A & Ehnfors, M. (2004) ‘Stroke and eating difficulties: long-term experiences’, Journal of Clinical Nursing,13(7), pp. 825–834. doi: 10.1111/j.1365-2702.2004.01023.x
Carter, N., Bryant-Lukosius, D., DiCenso, A., Blythe, J. & Neville, A. J. (2014) ‘The use of triangulation in qualitative research’, Oncology Nursing Forum, 41(5), pp. 545–547. doi: 10.1188/14.ONF.545-547
Critical Appraisal Skills Programme (2021) CASP Checklist: 10 questions to help you make sense of a Qualitative research. Available at: https://casp-uk.b-cdn.net/wp-content/uploads/2018/03/CASP-Qualitative-Checklist-2018_fillable_form.pdf (Accessed: 17 January 2022)
Daher, M. Carre, D., Jaramillo, A., Olivares, H. & Tomicic, A. (2017) ‘Experience and Meaning in Qualitative Research: A Conceptual Review and a Methodological Device Proposal’, Forum Qualitative Social Research, 18(3), pp. 18. doi: 10.17169/FQS-18.32696
Drozdz, D., Mancopes, R., Silva, A. M. T. & Reppold, C. (2014) ‘Analysis of the Level of Dysphagia, Anxiety, and Nutritional Status Before and After Speech Therapy in Patients with Stroke’, International Archives of Otorhinolaryngology, 18(2), pp. 172–177. doi: 10.1055/s-0033-1364169
Dworkin, S. L. (2012) ‘Sample Size Policy for Qualitative Studies Using In-Depth Interviews’, Archives of Sexual Behaviour, 41(6). doi: 10.1007/s10508-012-0016-6
ESNEFT (2022) About ESNEFT. Available at: https://www.esneft.nhs.uk/about-us/about-esneft/ (Accessed: 17 May 2022)
Eltringham, S. A., Pownall, S., Bray, B., Smith, C. J., Piercy, L. & Sage K. (2019) ‘Experiences of dysphagia after stroke: an interview study of stroke survivors and their informal caregivers’, Geriatrics, 4(4). doi: 10.3390/geriatrics4040067
Engel, R. J. & Schutt, R. K. (2005) The practice of research in social work. Thousand Oaks, CA: Sage Publications.
Faber, J. & Fonseca, L. M. (2014) ‘How small sample size influences research outcomes’, Dental Press Journal of Orthodonctics, 19(4), pp. 27–29. doi: 10.1590/2176-9451.19.4.027-029.ebo
Fernandez, M. G., Ottenstein, L., Atanelov, L. & Christian, A. B. (2013) ‘Dysphagia after stroke: an overview’, Current Physical Medicine and Rehabilitation Reports, 1(3), pp. 187–196. doi: 10.1007/s40141-013-0017-y
Forder, J., Vadean, F., Rand, S. & Malley, J. (2017) ‘The impact of long-term care on quality of life’, Health Economics, 27(3). doi: 10.1002/hec.3612
Green, J. & Thorogood, N. (2018) Qualitative Methods for Health Research. (4th Eds) London: Sage Publications Ltd.
Health and Care Professions Council (2022) Standards of Continuing Professional Development. Available at: https://www.hcpc-uk.org/standards/standards-of-continuing-professional-development/ (Accessed: 2 December 2021)
Hellden, J., Bergstrom, L. & Karlsson, S. (2018) ‘Experiences of living with persisting post-stroke dysphagia and of dysphagia management – a qualitative study’, International Journal of Qualitative Studies in Health and Well-being, 13(1). doi: 10.1080/17482631.2018.1522194
Holland, K. and Rees, C. (2010). Nursing evidence-based practice skills. USA: Oxford University Press.
Hong, C. J., Kaur, M. N., Farrokhyar, F. & Thoma, A. (2015) ‘Accuracy and completeness of electronic medical records obtained from referring physicians in a Hamilton, Ontario, plastic surgery practice: A prospective feasibility study’, Plastic Surgery, 23(1), pp. 48–50. doi: 10.4172/plastic-surgery.1000900
Hong, D. G. & Yoo, D. H. (2017) ‘A comparison of the swallowing function and quality of life by oral intake level in stroke patients with dysphagia’, Journal of Physical Therapy Science, 29(9), pp. 1552–1554. doi: 10.1589/jpts.29.1552
Jacobsson, C., Axelsson, K., Osterlind, P. O. & Norberg, A. (2000) ‘How people with stroke and healthy older people experience the eating process’, Journal of Clinical Nursing, 9(2), pp. 255–264. doi: 10.1046/j.1365-2702.2000.00355.x
Jason, L. and Glenwick, D. (2016). Handbook of methodological approaches to community-based research: Qualitative, quantitative, and mixed methods. New York: Oxford University Press.
Joanna Briggs Institute (2017) Checklist for Analytical Cross Sectional Studies. Available at: https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Analytical_Cross_Sectional_Studies2017_0.pdf (Accessed: 17 January 2022)
Johnson, J. L., Adkins, D. & Chauvin, S. (2020) ‘A Review of the Quality Indicators of Rigor in Qualitative Research’, American Journal of Pharmaceutical Education, 84(1). doi: 10.5688/ajpe7120
Journal of Stroke (2022) Aims and Scope. Available at: https://j-stroke.org/about/ (Accessed: 17 May 2022)
Jungmann, S. M. & Witthoft, M. (2020) ‘Health anxiety, cyberchondria, and coping in the current COVID-19 pandemic: Which factors are related to coronavirus anxiety?’, Journal of Anxiety Disorders, 73. doi: 10.1016/j.janxdis.2020.102239
Kim, DY., Park, HS., Park, SW. & Kim, JH. (2020) ‘The impact of dysphagia on quality of life in stroke patients’, Medicine, 99(34). doi: 10.1097/MD.0000000000021795
Kjaersgaard, A. & Pallesen, H. (2020) ‘First-hand experience of severe dysphagia following brainstem stroke: two qualitative cases’, Geriatrics, 5(1). doi: 10.3390/geriatrics5010015
Krans, J., Bree, J. D. & Bryant, R. A. (2013) ‘Autobiographical memory bias in social anxiety’, Memory, 22(8). doi: 10.1080/09658211.2013.844261
Langdon, C. & Blacker, D. (2010) ‘Dysphagia in Stroke: A New Solution’, Stroke Research and Treatment, 2010(9), pp. 1–6. doi: 10.4061/2010/570403
Li, C., Qiu, C., Shi, Y., Yang, T., Shao, X. & Zheng, D. (2021) ‘Experiences and perceptions of stroke patients living with dysphagia: a qualitative meta-synthesis’, Journal of Clinical Nursing, pp. 1–12. doi: 10. 1111/jocn.15995
Long, H. A., French, D. P. & Brooks, J. M. (2020) ‘Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis’, Research Methods in Medicine & Health Sciences, 1(1), pp. 31–42. doi: 10.1177/2632084320947559
Matua, G. A. & Der-Wal, D. M. V. (2015) ‘Differentiating between descriptive and interpretive phenomenological research approaches’, Nurse Researcher, 22(6), pp. 22–27. doi: 10.7748/nr.22.6.22.e1344
Martin-Harris, B. & Jones, B. (2008) ‘The Videofluorographic Swallowing Study’, Physical Medicine and Rehabilitation Clinics of North America, 19(4), pp. 769–785. doi: 10.1016/j.pmr.2008.06.004
McHorney, C., Robbins, J., Lomax, K., Rosenbek, J. C., Chignell, K., Kramer, A. E. & Bricker, D. E. (2002) ‘The SWAL–QOL and SWAL–CARE Outcomes Tool for Oropharyngeal Dysphagia in Adults: III. Documentation of Reliability and Validity’, Dysphagia, 17, pp. 97–114. Available at: https://link.springer.com/article/10.1007/s00455-001-0109-1 (Accessed: 14 February 2022)
McMullin, C. (2021) ‘Transcription and Qualitative Methods: Implications for Third Sector Research’, Nature Public Health Emergency Collection, 10, pp. 1–14. doi: 10.1007/s11266-021-00400-3
Medin, J., Larson, J., Arbin, MV., Wredling, R. & Tham, K. (2010) ‘Elderly persons’ experience and management of eating situations 6 months after stroke’, Disability and Rehabilitation, 32(16), pp. 1346–1353. doi: 10.3109/ 09638280903514747
Moloney, J. & Walshe, M. (2017) ‘“I had no idea what a complicated business eating is…”: a qualitative study of the impact of dysphagia during stroke recovery’, Disability and Rehabilitation, 40(13), pp. 1524–1531. doi: 10.1080/09638288.2017.1300948
National Institute for Health and Care Research (2022) Funding Opportunities. Available at: https://www.nihr.ac.uk/researchers/funding-opportunities/ (Accessed: 17 May 2022)
Noble, H. & Smith, J. (2015) ‘Issues of validity and reliability in qualitative research’, Evidence-Based Nursing, 18(2), pp. 34–35. doi: 10.1136/eb-2015-102054
Palinkas, L. A., Horwitz, S. M., Green, C. A., Wisdom, J. P., Duan, N. & Hoagwood, K. (2015) ‘Purposeful sampling for qualitative data collection and analysis in mixed method implementation research’, Administration and Policy in Health, 42(5), pp. 533–544. doi: 10.1007/s10488-013-0528-y
Payscale (2022) Average Transcriber Hourly Pay in United Kingdom. Available at: https://www.payscale.com/research/UK/Job=Transcriber/Hourly_Rate (Accessed: 22 April 2022)
Perry, L. & McLaren, S. (2003) ‘Coping and adaptation at six months after stroke: experiences with eating disabilities’, International Journal of Nursing Studies, 40(2), pp. 185–195. doi: 10.1016/s0020-7489(02)00060-3
PRISMA (2009) PRISMA Flow Diagram. Available at: http://prisma-statement.org/documents/PRISMA%202009%20flow%20diagram.pdf (Accessed: 21 December 2021)
Pithon, M. M. (2013) ‘Importance of the control group in scientific research’, Dental Press Journal of Orthodontics, 18(6), pp. 13–14. doi: 10.1590/S2176-94512013000600003
Pontes, E. S., Amaral, A. K., Rego, F. L., Azevedo, E. M & Silva, P. O. (2017) ‘Quality of life in swallowing of the elderly patients affected by stroke’, Arquivos de Gastroenteral, 54(1), pp. 27–32. doi: 10.1590/S0004-2803.2017v54n1-05
Royal College of Speech and Language Therapy (2021) Dysphagia – Guidance. Available at: https://www.rcslt.org/members/clinical-guidance/dysphagia/dysphagia-guidance/ (Accessed: 3 December 2021)
Royal College of Speech and Language Therapy (2022a) Research Advice and Support. Available at: https://www.rcslt.org/members/research/advice-and-support/#section-6 (Accessed: 17 May 2022)
Royal College of Speech and Language Therapy (2022b) Surveys. Available at: https://www.rcslt.org/help-and-support/surveys/#:~:text=for%20Disseminating%20Surveys-,Introduction,a%20limited%20number%20of%20surveys. (Accessed: 17 May 2022)
Rutakuma, R., Mugisha, J. O., Bernays, S., Kabunga, E., Tumwekwase, G., Mbonye, M. & Seeley, J. (2020) ‘Conducting in-depth interviews with and without voice recorders: a comparative analysis’, Qualitative Research, 20(5), pp. 565–581. doi: 10.1177/1468794119884806
Scheel, C., Mecham, J., Zuccarello, V. & Mattes, R. (2018) ‘An evaluation of the inter-rater and intra-rater reliability of OccuPro’s functional capacity evaluation’, Work (Reading, Mass), 60(3), pp. 465–473. doi: 10.3233/WOR-182754
Seymour, J. (2017) ‘The Impact of Public Health Awareness Campaigns on the Awareness and Quality of Palliative Care’, Journal of Palliative Medicine, 20 (S1). doi: 10.1089/jpm.2017.0391
Smith, J. A. & Osborn, M. (2015) ‘Interpretative phenomenological analysis as a useful methodology for research on the lived experience of pain’, British Journal of Pain, 9(1), pp. 41–42. doi: 10.1177/2049463714541642
Smith, R., Bryant, L. and Hemsley, B. (2023). ‘The true cost of dysphagia on quality of life: The views of adults with swallowing disability’. International Journal of Language & Communication Disorders, 58(2), pp. 451–466. doi: 10.1111/1460-6984.12804
Stroke Association (2021) Swallowing Problems. Available at: https://www.stroke.org.uk/effects-of-stroke/physical-effects-of-stroke/swallowing-problems (Accessed: 26 December 2021)
Stroke Association (2022a) Take part in research. Available at: https://www.stroke.org.uk/research/get-involved-research/take-part-in-research (Accessed: 17 May 2022)
Stroke Association (2022b) Our Funding Schemes. Available at: https://www.stroke.org.uk/research/our-funding-schemes (Accessed: 17 May 2022)
Threats, T. T. (2007) ‘Use of the ICF in Dysphagia Management’, Seminars in Speech and Language, 28(4), pp. 323–333. doi: 10.1055/s-2007-986529
Triggs, J. & Pandolfino, J. (2019) ‘Recent advances in dysphagia management’, F1000 Research, 8, p. 1527. doi: 10.12688/f1000research.18900.1
United Kingdom Research and Innovation (2022) Apply for Funding. Available at: https://www.ukri.org/apply-for-funding/ (Accessed: 17 May 2022)
University of Essex (2022a) Ethical Aprroval: resources for applicants. Available at: https://www.essex.ac.uk/staff/research-governance/ethical-approval-resources-for-applicants (Accessed: 17 May 2022)
Univeristy of Essex (2022b) Research and Enterprise Office Team. Available at: https://www.essex.ac.uk/student/professional-services/research-enterprise-office-team (Accessed: 17 May 2022)
Vasileiou, K., Barnett, J., Thorpe, S. Young, T. (2018) ‘Characterising and justifying sample size sufficiency in interview-based studies: systematic analysis of qualitative health research over a 15-year period’, BMC Medical Research Methodology, 18(1). doi: 10.1186/s12874-018-0594-7
Waite, M. (2009) Oxford Thesaurus of English. (3rd Eds) Oxford: Oxford University Press.
Wiley Online Library (2022) Aims and Scope. Available at: https://onlinelibrary.wiley.com/journal/14606984 (Accessed: 17 May 2022)
Willis, J. W. & Nilakanta, R. (2007) Foundations of Qualitative Research: Interpretive and Critical Approaches. 1st edition. Los Angeles: SAGE Publications.
Wilson, P. M., Petticrew, M., Calnan, M. W. & Nazareth, I. (2010) ‘Disseminating research findings: what should researchers do? A systematic scoping review of conceptual frameworks’, Implementation Science, 5. p. 91. doi: 10.1186/1748-5908-5-91
World Health Organisation (2022a) WHOQOL: Measuring Quality of Life. Available at: https://www.who.int/tools/whoqol (Accessed: 24 January 2022)
World Health Organisation (2022b) International Classification of Functioning, Disability and Health (ICF). Available at: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health (Accessed: 26 January 2022)
Appendices
Appendix 1
Appendix 2
Glossary:
| Term | Definition | Reference |
|---|---|---|
| Convenience sampling | Sampling method whereby participants are selected based on being close at hand to the researcher. | (Bryman, 2008) |
| Descriptive phenomenology | A method to explore and describe the lived experiences of individuals. | (Bryman, 2008) |
| Dysphagia | Medical term for swallowing difficulties. | (Langdon & Blacker, 2010) |
| Ethnography | The study of individuals ad their culture, including customs, beliefs, habits, and mutual differences. | (Aveyard, 2019) |
| Grounded theory | A qualitative methodology that enables researchers to generate theory. | (Aveyard, 2019) |
| Interpretivism | An approach that studies humans in terms of their subjective experiences, views, opinions, and emotions. | (Aveyard, 2019) |
| Interpretive phenomenological analysis | Form of qualitative data analysis that seeks to provide detailed examinations of personal lived experiences. | (Bryman, 2008) |
| Interpretivist phenomenology | A method to explore and understand the lived experiences of individuals. | (Bryman, 2008) |
| Inter-subjective reflexivity | How the relationship between the participant and researcher may influence the research. | (Bryman, 2008) |
| Maximum variation sampling | Sampling method whereby researcher attempts to collect participants from the widest range of perspectives on a certain topic. | (Bryman, 2008) |
| Oropharyngeal dysphagia | Swallowing difficulty occurring in the mouth and/or throat. | (Moloney & Walshe, 2017) |
| Phenomenology | Study of lived experiences. | (Aveyard, 2019) |
| Purposeful sampling | Sampling method whereby participants are selected based on meeting a certain characteristic. | (Bryman, 2008) |
| Quality of life | An individual’s perception of their living with regards to their expectations, concerns, goals, and standards. | (World Health Organisation, 2022a) |
| Random selection | Sampling method whereby by participants are selected at random to have an equal opportunity of being selected. | (Bryman, 2008) |
| Recall bias | Memory impacts what information is remembered. | (Bryman, 2008) |
| Reflexivity | When an individual examines how his or her own experiences, thoughts, opinions, and feelings may influence a situation. | (Bryman, 2008) |
| Stroke | Blood supply to part of the brain is disrupted. | (Moloney & Walshe, 2017) |
| Swallowing function test | A test used to measure the level of swallowing function. | (Hong & Yoo, 2017) |
| Swallowing quality of life questionnaire | A quantitative 44-item tool that assesses and measures quality of life for individuals with oropharyngeal dysphagia. | (Pontes et al, 2017) |
| Videofluoroscopic Dysphagia Scale | Used to predict the long-term prognosis of dysphagia patients following stroke. | (Kim et al, 2020) |
| Videofluoroscopy | A swallowing x-ray to assess an individual’s swallowing ability. | (Kim et al, 2020) |
| Verstehen | To form an empathetic and deep understanding of human behaviour. | (Bryman, 2008). |
Appendix 3
Interview Topic guide - Preset topics and open questions for semi-structured interviews:
Topics
Environment
Mental well-being
Physiology
Healthcare professionals
Coping / adaptation
Dysphagia
Employment
Pre-set questions
(One preset open question for each topic, and then researcher would improvise follow-up questions)
What has your environment been like, such as interaction with other people, relationships and social situations since your swallowing has changed?
How have you been feeling since your swallowing has changed?
What has it been like to interact with health / care services since your swallowing changed?
What does dysphagia mean to you?
What does it physically feel like to have dysphagia?
Appendix 4
Research Proposal
Questions, Aims & Objectives
Research Questions:
Primary question: What are the lived experiences of people living with long-term post-stroke dysphagia in the community?
Secondary question: How can the experiences of people living with long-term post-stroke dysphagia in the community inform others about how quality of life is impacted?
Research aims:
The aim of this study is to:
Understand and explore the long-term lived experiences of post-stroke dysphagia for those living in the community
Understand how quality of life is impacted by post-stroke dysphagia
Generate new ideas by addressing the research gap identified in the above literature review
Inform SLT practices and commissioning of services of these experiences to provide higher quality and evidence-based care
Add to the knowledge base regarding the lived experiences of patients with post-stroke dysphagia
Research objectives:
To describe the lived experiences of people living with long-term post-stroke dysphagia in the community
To explore how long-term post-stroke dysphagia could influence the different aspects of QoL such as the environment, mental well-being, and physiology
Copyright Statement
©Zainab Khatun Hussain. This article is licensed under a Creative Commons Attribution 4.0 International Licence (CC BY).